
I was about to put a PFT report I’d been reviewing in my outbox when I noticed something odd about the flow-volume loop.
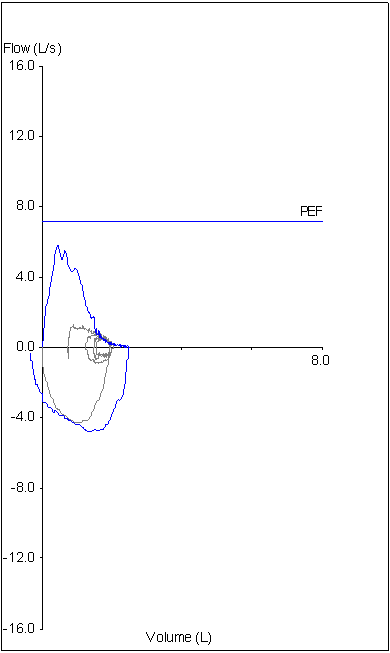
What I saw was that the final inspiration of the FVC maneuver had ended to the left of the initial inspiration. This means a couple of thing, first and foremost that the FIVC was larger than the FVC and that the FVC was likely underestimated because the patient hadn’t really taken a full inspiration prior to exhaling. I had already looked at the raw data for the patient’s spirometry results for other reasons but I pulled them up again to see if I had missed something.
What I saw was that the spirometry test with the best FVC, FEV1, PEF and expiratory time was the one that had been selected for reporting. I also saw that all of the patient’s spirometry results were fairly uniform and met the ATS/ERS requirements for repeatability. Despite the fact that the FVC in every effort was likely submaximal the patient had managed to perform the FVC maneuvers with remarkable similarity.
What I didn’t see however, was any visible indication that the FIVC was larger than the FVC (and it’s important to note that the software module I use to review spirometry results is the same that’s used to perform the test in the first place).
I had to page down a bit in the tabular results to see that yes, the FIVC was significantly larger than the FVC. In one sense this didn’t make a difference for this particular patient’s report because I had already noted that the SVC from the patient’s lung volume test was larger than the FVC and that FEV1/SVC ratio was reduced which indicated the presence of airway obstruction. The FIVC and SVC were in fact essentially identical so the FEV1/VC wasn’t going to be any different.
When I review a report that has lung volumes and/or a DLCO along with spirometry I always compared the SVC from the lung volumes and the inspired volume from the DLCO with the FVC. If either are larger than the FVC I recalculate the FEV1/VC ratio to see if it is low. Patients with airway obstruction often have a significantly larger SVC or Inspired Volume than their FVC and this is likely because of the airway compression that occurs during a forced expiratory effort that doesn’t occur during a more relaxed effort.
What I tend to forget however (and this is a good reminder), is that the FVC can also be underestimated because of a suboptimal inspiration. Detecting an inadequate inspiratory effort tends to be difficult because there usually isn’t any good indication that it is happening. To some extent you can tell through body language or from irreproducible results that a patient isn’t inhaling correctly but unlike a suboptimal expiration there are no objective criteria for a suboptimal inspiration. In this patient’s case because their flow-volume loops, volume-time curves and numerical results all met quality and repeatability criteria there was no particular indication at all that the inspiration was lower than it should have been.
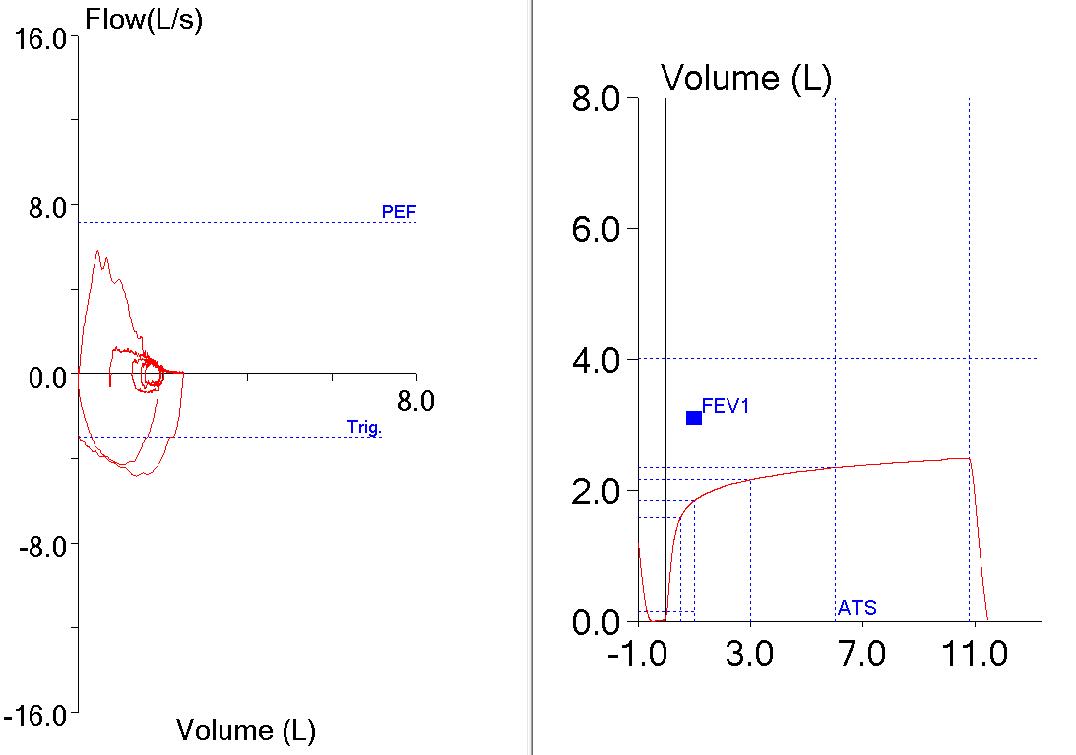
What is important about all this is that when I review the patient’s raw spirometry test data (and more importantly when the test is being performed) it is very difficult to see that the FIVC is larger than the FVC. This is because all of the inspiratory flow-volume loop and volume-time data are cut off at the point of the initial peak inspiration for the FVC effort. Why is this happening? Strictly speaking this is a decision made by a programmer or other software designer and not from anything in the ATS/ERS standards for spirometry, so the blame, if there is any, can be placed on the manufacturer of our test equipment.
Why did the larger inspiratory effort show up on the report but not when I reviewed the raw spirometry data? Maybe there were different design specifications, or maybe because of an oversight, or because the graph software was written by a different programmer or maybe even because of sloppy programming. Regardless of the reason it was fortuitous because otherwise I wouldn’t have noticed it at all. But this also points out a blind spot we may all have. Look in any textbook or journal article and you will see that it is a standard convention that the position of the flow-volume loop in its graph is always determined by the initial inspiratory effort and not by any subsequent inhalation. This is probably a mistake on our part.
The ATS/ERS recommendation is to use the largest VC, regardless of the source, when calculating the FEV1/VC ratio. For this reason, the maximal flow-volume loop should be positioned on its graph relative to the largest inspiration, not the initial inspiration. If this was done, the flow-volume loop for this patient would have looked like this:
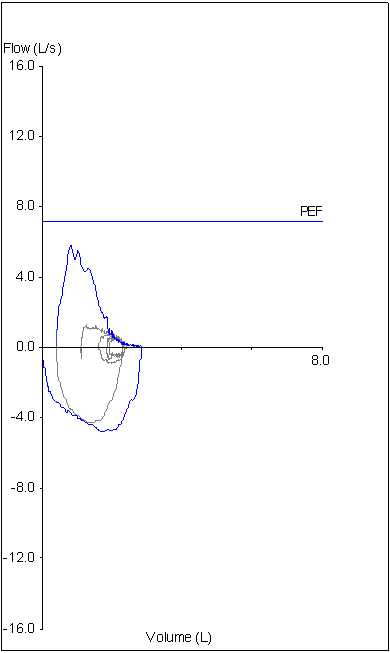
When displayed this way it would have been immediately evident that the initial inspiration was inadequate and for this reason it would be my recommendation that this should be the standard approach for graphing flow-volume loops. This may be a problem unique to the manufacturer of my lab’s test equipment but I’d be willing to bet it isn’t. I don’t have access to any other manufacturer’s test equipment so I can’t verify this in any way but since “everybody” knows how flow-volume loops are “supposed” to be graphed I’d be inclined to guess it’s pretty universal.
We have a limited amount of space on our reports and there are many spirometry values we don’t report both for the sake of clarity and the sake of brevity. FIVC is not a value we report and in fact we look at it only rarely. This is due to the fact that almost always the FIVC is less than or at best equal to the FVC so it doesn’t seem like it’s particularly important. This doesn’t mean that an FIVC can’t be an important clue when assessing spirometry test quality. It also doesn’t means that the FIVC should be overlooked when searching for the largest VC for the FEV1/VC ratio. Most importantly though, it means that the FIVC shouldn’t be hidden by artificially limiting how much of it is displayed on a flow-volume loop when it is being reviewed and most particularly when the test is being performed.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.