Well, not necessarily anything, although as usual that depends on the circumstances. Recently I was contacted by an individual who was concerned that their DLCO had decreased from 120% of predicted to 99% of predicted. They also mentioned that their DLCO results have normally ranged from 117% to 140% of predicted over the last 9 months.
More interestingly however, they said that
“the technician told me before I even took the test that anything over 100% for DLCO is essentially a testing error.”
Wow. That statement is wrong on so many levels it’s hard to know where to start but I’ll give it a shot anyway.
First, there are a variety of DLCO reference equations. The ATS/ERS guidelines recommends that PFT Labs pick the reference values that most closely matches their patient population but how this is done is left to individual labs. There are at least a couple dozen DLCO reference equations to choose from and probably about a half dozen of these are in common use in PFT labs around the world.
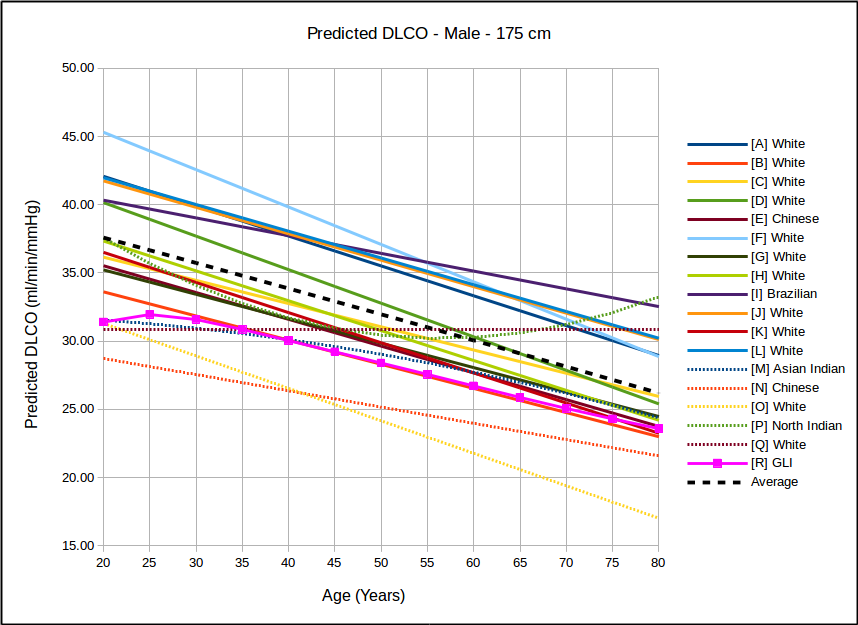
Because no patient population is ever going to precisely match those of a study this means that DLCO results are going to tend to be above or below 100% of predicted depending on which reference equation the lab is actually using. This also means that if results from otherwise normal subjects are mostly above or mostly below 100% of predicted then the wrong reference equations are being used.
Moreover, if a lab selects a DLCO reference equation based on the expectation that everybody will be either 100% of predicted or less, that is also wrong. DLCO, like all other pulmonary function results, follows a normal, bell-shaped distribution.
Reference equations are used to calculate the mean value and this means that approximately half the study population is above the mean and half is going to be below it. Admittedly most study subjects aren’t going to be too far away from the mean, but as an example Miller et al (H in the above graph) is one of the more commonly used DLCO reference equations. They did not include a lower limit of normal (LLN) in their original paper but did include extensive statistics on the study population. Although I have some significant disagreements with this approach many labs calculate the LLN for DLCO as:

For Miller et al the SEE (Standard Error of the Estimate) x 1.645 is 7.99 ml/min/mm Hg. The upper limit of normal (ULN) can be calculated the same way,

Since the predicted DLCO for a 50 year old, 175 cm male is 30.77 ml/min/mmHg, the ULN for the same patient would be 38.76 ml/min/mmHg, but that value is 126% of predicted. So it’s easily possible to be within normal limits, but above 120% of predicted.
Probably far more pertinent to the person who contacted me about this issue (who has a tentative diagnosis of reactive airways disease and a BMI > 30), is that DLCO is frequently elevated in both asthma and in obesity. In a study of 245 patients with a DLCO >140% of predicted, Saydain et al found that most of the patients had a diagnosis of either asthma, obesity, or both. The reasons for this are unclear but subjects with asthma have been noted to have increased airway vascularization, and therefore an elevated capillary surface area in the lung. Other researchers have noted that asthma is associated with an elevated perfusion of the lung apices. And numerous other researchers have shown that obese individuals have an elevated capillary blood volume and an elevated cardiac output.
So, is an elevated DLCO abnormal in these individuals? Probably not since no one has shown that an elevated DLCO is an adverse clinical findings in either asthma or obesity but in particular it also means that an elevated DLCO should not be dismissed as a testing error in these patients.
A much smaller minority in Saydain et al’s study had pulmonary hemorrhage, polycythemia or left-to-right shunting. These are adverse clinical findings and for this reason, even more so than asthma or obesity, an elevated DLCO should not be ignored as a testing error.
This is not to say that there aren’t DLCO testing errors that lead to an elevated DLCO and I’d be interested in what that lab’s policy was on checking test systems when a patient has an elevated DLCO.
The DLCO test is sensitive to the pulmonary capillary blood volume and this can be affected by excess resistance during inspiration and by a Müller maneuver (inspiratory effort against a closed mouthpiece) both of which cause a negative intrapulmonary pressure and act to increase the capillary blood volume. The 2017 ERS/ATS DLCO standards explicitly mentions the need to avoid a Müller maneuver and the standard’s equipment specifications includes the statement that:
“Circuit resistance must be <1.5 cmH2O·L−1·s−1 up to 6 L·s−1 flow. If a demand-flow regulator is used on a compressed test gas cylinder, the maximal inspiratory pressure required for 6 L·s−1 inspiratory flow through both the circuit and the valve must be <9 cmH2O.”
The demand valve specifications in the ERS/ATS standard are not based on any particular evidence however, and are essentially a way to grandfather-in existing test systems. To my knowledge the effect that an inspiratory pressure of -9 cm H2O has on DLCO has not been studied (although at least one equipment manufacturer I’m familiar with has designed their DLCO systems without demand valves specifically because of their concerns with this issue). Regardless of whether or not an inspiratory pressure of -9 cm H2O affects DLCO, a sticking demand valve will significantly increase a subject’s inspiratory pressure. This will probably increase the measured DLCO as well and should be considered a testing error.
Interestingly, although the ERS/ATS standard acknowledges that exercise affects pulmonary capillary blood volume (due to an elevated cardiac output), other than stating that:
“…the subject must be seated comfortably throughout the test procedure…”
it does not specify any pre-test waiting period although a minimum 4 minute between-test waiting period is recommended. This waiting period however, is intended to allow for adequate elimination of test gas from the lungs and not as a way to ensure the patient is in a resting state.
Note: I’ve used the effects of exercise as a talking point when teaching students about DLCO testing. To do this I perform a DLCO on a student after they’ve sat quietly for several minutes. Next I get the test system set up for another DLCO test but first I have them walk briskly up and down the hallway for several minutes, then sit down and immediately perform another DLCO. Their second, post-exercise, DLCO is almost always at least 15% to 30% higher than their resting DLCO.
Most of the time however, testing errors such as a valve and tubing failures, a reduced inspiratory volume, a reduced breath-holding time or an inadequate or mistimed alveolar sample tend to cause a decrease in DLCO, not an increase. Having said that, I’ve run across problems with gas analyzers that can cause an elevated DLCO, and these can be hard to detect because they are often transient. The same applies to computer glitches of one kind or another.
I remain somewhat baffled about the statement that any DLCO over 100% of predicted is a testing error. What is it based on and is it blaming the patient or the test system? If the technician and the lab actually believes it, then why were the elevated DLCO’s reported anyway?
Unfortunately, I think that it’s more likely the technician was pontificating about a subject they did not understand. It’s worse if they were parroting a statement made by a co-worker, their manager or their medical director since that points to a systemic lack of understanding about testing issues and idiosyncrasies which is (also unfortunately) more common than it should be.
In my lab we get DLCO’s >140% of predicted several dozen times a year and >120% of predicted far more frequently. I always review the raw data for these tests but then I review the raw data for all DLCO tests so they are not singled out in any particular way. I don’t find any apparent testing errors with elevated DLCO results any more often than I do with regular DLCO results. I’ve also been aware of the association between asthma and elevated DLCO’s for more than 30 years so I’ve never seen any reason not to report them.
The original question however, was whether a decrease in DLCO from 120% of predicted to 99% of predicted was abnormal and I don’t have a good answer for that. Partly this is because the intrasession reproducibility of elevated DLCOs has not been studied. Partly it’s because the specific causes of an elevated DLCO in a given individual are poorly understood and for this reason it’s not possible to say whether changes like this are clinically significant or not.
It’s also unclear why this individual is having their DLCO tested so frequently. The only working diagnosis they have is mild shortness of breath and possible reactive airways disease, and those are not good reasons to repeat DLCO tests so frequently. Does their physician suspect something they haven’t yet shared or is it just the policy that DLCO is tested with each patient visit? I’m left with a number of questions but at least I was able to let them know that an elevated DLCO is actually normal for many individuals and not a testing error.
References:
Graham BL, Brusasco V, Burgos F, et al. 2017 ERS/ATS standards for single-breath
carbon monoxide uptake in the lung. Eur Respir J 2017; 49: 1600016.
Miller A, Thornton JC, Warshaw R, Anderson H, Teirstein AS, Selikoff IJ. Single breath diffusing capacity in a representative of Michigan, a large industrial state. Am Rev Resp Dis 1983; 127: 270-277.
Saydain G, Beck KC, Decker PA, Cowl CT, Scanlon PD. Clinical significance of elevated diffusing capacity. Chest 2004; 125: 446-452.
Tanaka H, Yamada G, Saikai T, Hashimoto M, Tanaka S, Suzuki K, Fujii M, Takahashi H, Abe S. Increased airway vascularity in newly diagnosed asthma using a high-magnification bronchovideoscope. Am J Respir Crit Care Med 2003; 168: 1495-1499.