The question that was actually posed to me a month or so ago was “when is RAW abnormal?” I didn’t have a good answer at the time since airway resistance (RAW) tests are not performed by my lab. The pulmonary physicians I work with don’t think that RAW is a clinically useful measurement and for a variety of reasons I don’t disagree with this. Nevertheless, RAW testing is routinely performed in many labs around the world so I thought it would be interesting to spend some time researching this.
When asking what’s normal the first issue is which RAW value are you talking about? The measurement of airways resistance using a body plethysmograph was first described by DuBois et al in 1956. Airway resistance (RAW) is the amount of pressure required to generate a given flow rate and is reported in cm H2O/L/Sec. A number of physiologists quickly found that the reciprocal of RAW, conductance (GAW), which is expressed as the flow rate for a given driving pressure (L/sec/cm H2O), was also a useful way to describe the pressure-flow relationship of the airways.
For technical reasons TGV (Thoracic Gas Volume) must be measured at the same time as RAW. It was soon noted that there was a relationship between RAW and TGV and that airway resistance decreased as lung volume increased.
Because the relationship between RAW, GAW and TGV was considered to be linear (and little affected by age), specific GAW (i.e. GAW/TGV, SGAW, expressed as L/sec/cm H2O/L) is considered to be independent of TGV (this is also more or less the case with the specific RAW (i.e. RAW/TGV, SRAW, expressed as cm H2O/L/sec/L) but this measurment is rarely made or reported). RAW and SGAW have since become the most common ways to report airway resistance but there are still occasional research papers where SRAW or GAW is reported instead.
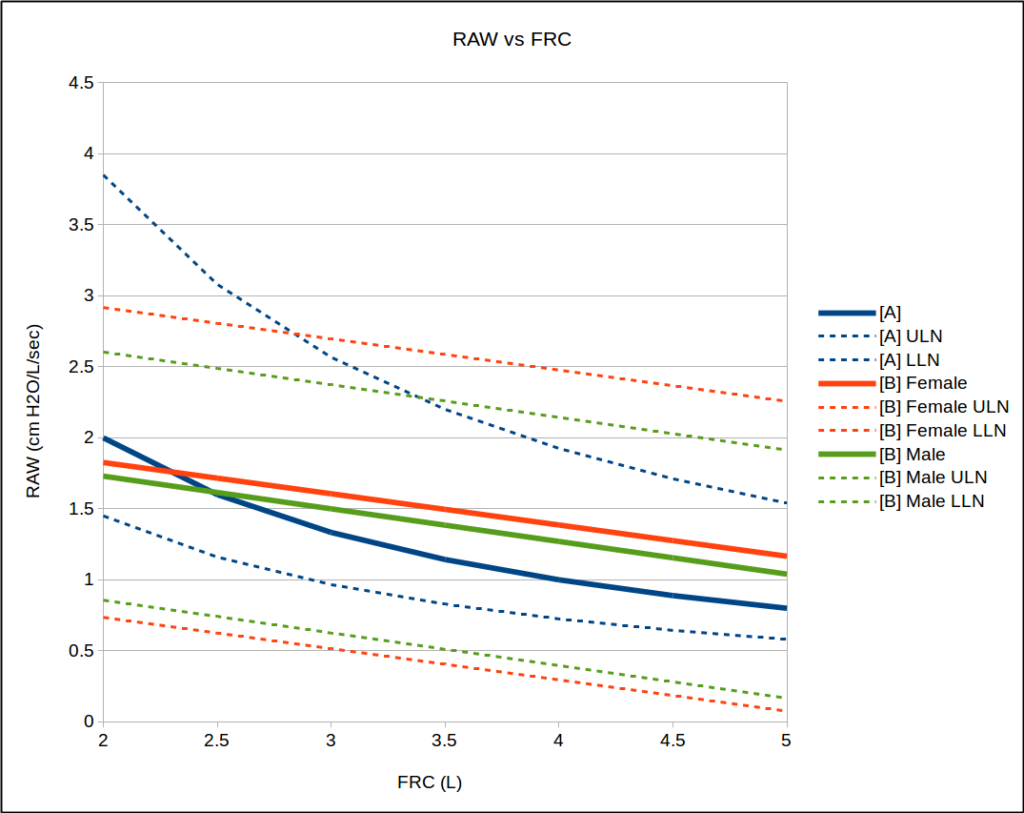
Although RAW has been studied many times there are actually very few articles that are concerned with normal values and the majority of them have reported just the mean and range for their study populations. The values for RAW and SGAW that Briscoe and Dubois published in 1958 were considered the gold standards for decades despite having a study population of only 26 individuals (10 F, 16 M, 8 children, 18 adults). In fact, there are almost no reference equations for RAW and SGAW and almost all of the pulmonary function textbooks I have on hand have published the normal range for RAW as 0.5 – 2.0 cm H2O/L/sec, and the normal range SGAW as 0.13 – 0.35 L/sec/cm H2O/L.
There is however, one recent population study (Marsh et al, 2006) with 212 individuals (Caucasian, 25-75 years, 51.9% male) that described the mean, ULN and LLN for SGAW and SRAW, and another (Gutierrez et al, 2004) with 627 individuals (Caucasian, 20-80 years, 47.8% male) that provided reference equations with a calculable ULN and LLN for RAW and SGAW.
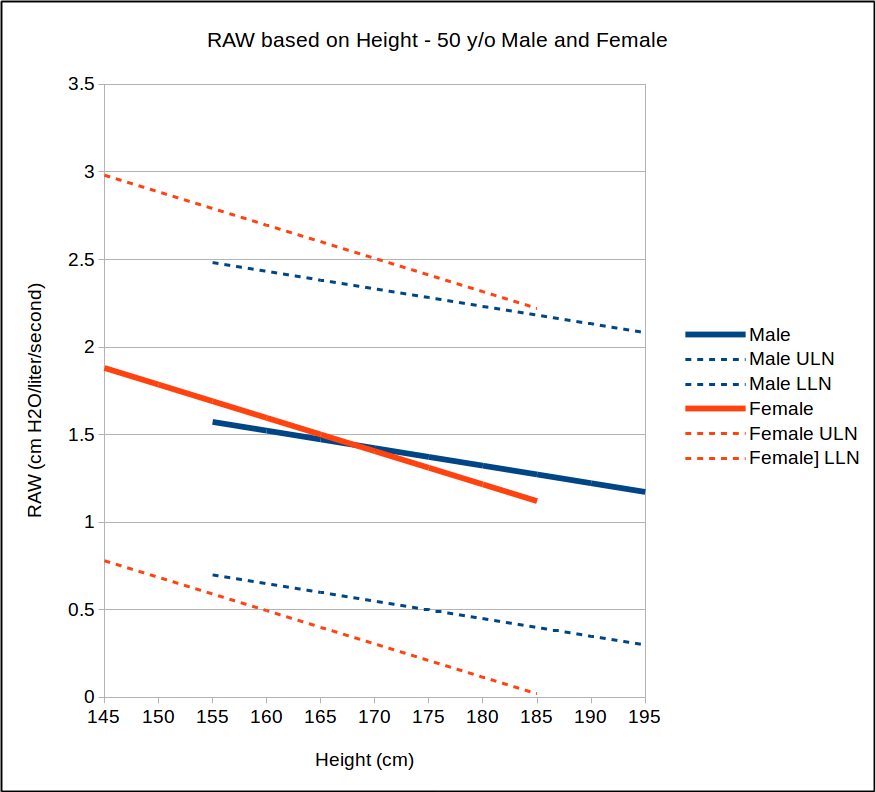
Not surprisingly given the relationship between TGV and RAW, the reference equations from Gutierrez et al show that RAW is primarily influenced by height.
They also showed that age has a slight effect for males, but was not considered significant for females.
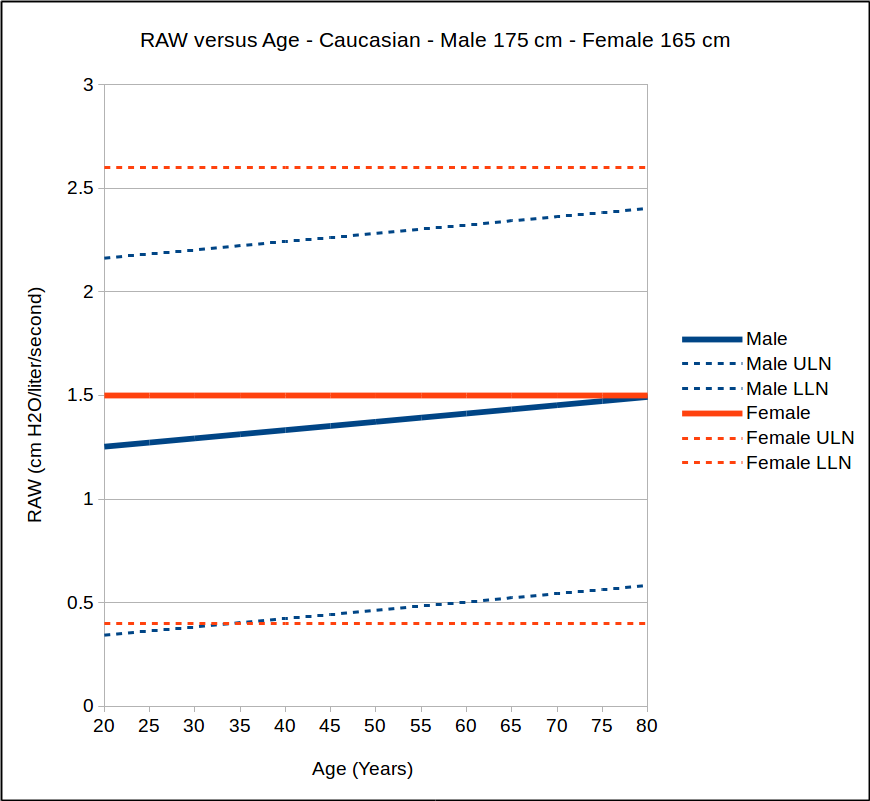
Given that SGAW is considered to be independent of TGV it is somewhat surprisingly to find that the Gutierrez reference equations show a distinct relationship with height. Marsh et al however, determined that height was not a factor. Both studies did not find age to be a factor for SGAW.
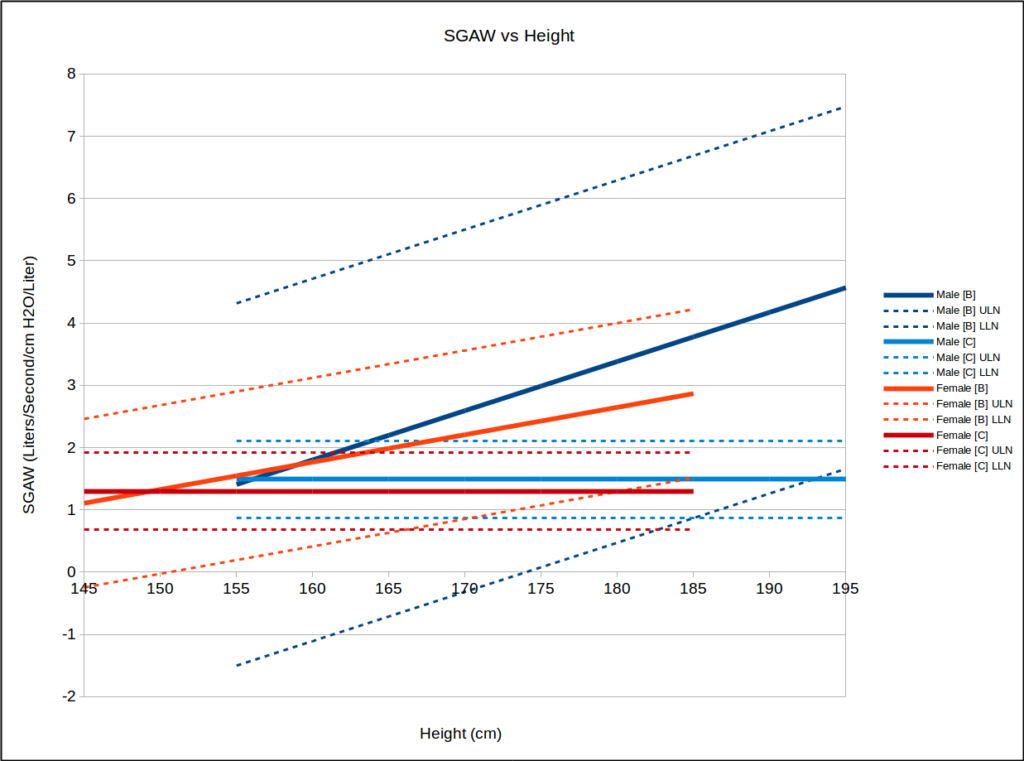
The Gutierrez reference equations have problems with both the male and the female LLN since at lower heights these values are negative. It should be noted that the SEE for SGAW was large relative to the mean value and the range of heights in the study population was not included.
There are fairly significant differences in values from the Gutierrez and Marsh reference equations, particular for taller individuals. This may be due to a smaller study population for the Marsh equations but also points out that the normal range for SGAW (and all of the other RAW measurements) still tends to be inconsistent from one study to another. As an example, a recent study of SGAW, RAW and airway obstruction indicated that within their clinical study population that consisted largely of patients with asthma and COPD the LLN for SGAW was 0.98. Another recent study however, showed that the normal range in SGAW for healthy subjects was 0.78 – 1.47.
So why are there some much difference in RAW and SGAW from otherwise comparable studies?
One factor that may affect the accuracy of measured RAW values may be the panting frequency. Although there are no ATS/ERS standards for panting frequency the original Dubois 1956 study used a panting frequency of 2 Hz. It has been variously reported in other studies however, as being anywhere from 1 – 3 Hz but far more frequently the panting frequency is unreported. The reason why this may be important is that Peslin et al showed an increase in RAW from 0.62 (±0.55) to 1.71 (±0.76) over a range of 0.25 to 3.0 Hz which the authors primarily attributed to inadequate BTPS correction in the software. An earlier study however, by Krell et al performed at two frequencies (approximately 1.5 and 3.0 Hz) did not show any difference in SGAW but the plethysmograph used in the study was constructed for research and all loops were analyzed manually.
In addition the flow interval over which RAW is usually measured (i.e. ±0.5 L/sec) is relatively arbitrary. It was originally ±1.0 L/sec in the original 1956 DuBois article but by 1958 the same investigators had changed the measurement range to ±0.5 L/sec because “The oscilloscope tracing was sometimes alinear, showing a tendency to curve at the extremes, presumably due to turbulent flow at higher flow rates.”
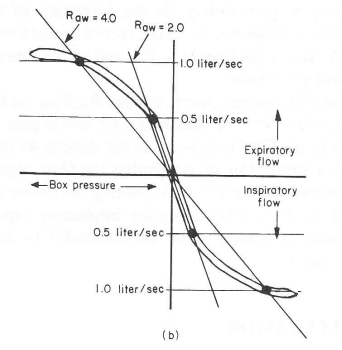
The middle section of the RAW loop may be more linear but a study by Lord and Edwards showed that RAW measured over ±0.5 L/sec was significantly more variable than when measured over ±1.0 L/sec and ±2.0 L/sec. In addition the RAW measured over ±0.5 L/sec is significantly greater than the RAW measured over ±2.0 L/sec.
It is also usually assumed that inspiratory and expiratory resistance in the range it is measured (i.e. at FRC and ±0.5 L/sec) are the same. This is reasonably true for individuals without airways disease but is not the case when significant airway obstruction is present.
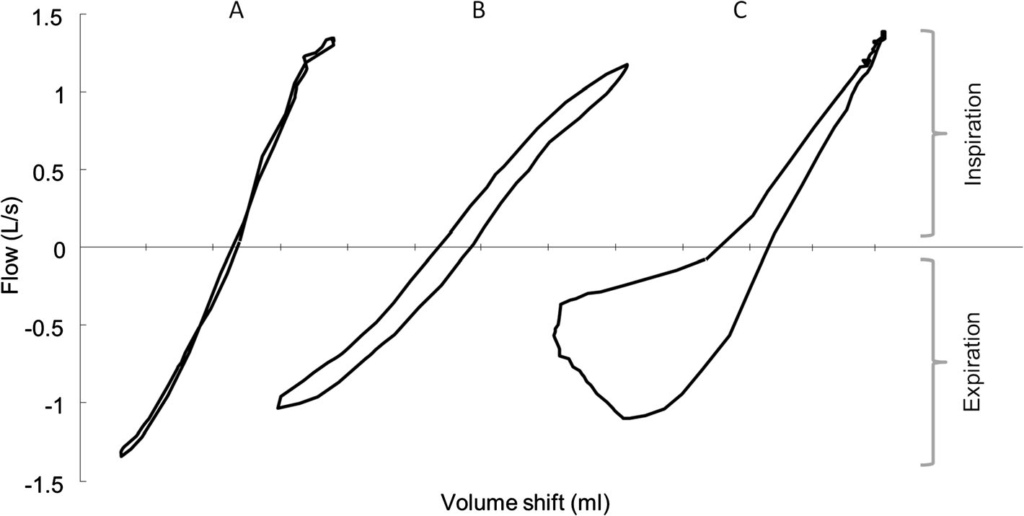
When the RAW loop opens up as shown above in figure C it becomes significantly less clear how RAW should be calculated. This probably does not affect the normal ranges for RAW but does make it more difficult to determine RAW in individuals with significant airway obstruction.
Another factor that I’ve not seen discussed is that there is a mild discrepancy between TGV and the lung volumes at which RAW is actually measured. Specifically, if measured correctly TGV should be essentially the same as FRC but although the tidal volumes that occur during the panting maneuver are likely small they occur above FRC. In addition, TGV is not always measured correctly and may be either above or below true FRC by some unknown amount. These errors are likely small but the effect they have on RAW and SGAW measurements has not been studied.
Finally, there is really no way to verify the accuracy of a RAW measurement (admittedly this is one of my chronic complaints but is more true of RAW than for most other pulmonary function tests). The days of manually taking the RAW angle from a storage oscilliscope or polaroid film and then hand calculating airway resistance are long gone. We are highly dependent on our lab software to not only record the raw test data accurately but to analyze it correctly. Spirometry, lung volume and DLCO measurements can be verified using simulators of one kind or another but there is no simulator for airway resistance. Also unlike spirometry, lung volumes and DLCO no inter-laboratory comparisons have ever been made of RAW measurements.
Given that the normal range for RAW is somewhat vague Ries and Clausen suggested that elevated RAW values be classified as:
| RAW: | Severity: |
| <2.8 | Normal |
| 2.8 – 4.5 | Mild obstruction |
| 4.5 – 8.0 | Moderate obstruction |
| >8.0 | Severe obstruction |
Miller et all made similar suggestions:
| RAW: | Severity: |
| <3.0 | Normal |
| 3.0 – 4.5 | Mild obstruction |
| 4.5 -8.0 | Moderate obstruction |
| 8.0 – 15.0 | Severe obstruction |
| >15.0 | Extreme obstruction |
Miller also made suggestions assessing the severity of SGAW measurements:
| SGAW: | Severity: |
| >0.114 | Normal |
| 0.114 – 0.070 | Mild obstruction |
| 0.070 – 0.040 | Moderate obstruction |
| 0.040 – 0.021 | Severe obstruction |
| <0.020 | Extreme obstruction |
Note: Millers values actually points out an interesting problem I’ve run across. Specifically, SGAW measurements reported from more than a couple decades ago are almost exactly 1/10th the magnitude of SGAW measurement reported currently (compare these to the predicted SGAW measurements from Gutierrez and Marsh). In many instances this is because the units used to report SGAW have changed to liters/sec/Kpa/liter (Kpa = 10.19 x cm H2O) but in other instances the SGAW measurements still use same units, i.e. liters/sec/cm H2O/liter. I’m sure there is an explanation somewhere but in the meantime it does make it difficult to compare results over time. FYI, RAW results reported in Kpa/L/sec are 1/10th those reported in cm H2O/L/sec so it’s important to keep track of which units are being reported.
Regardless of whether airway resistance is reported as RAW or SGAW, the normal range is comparatively much larger than it is for FEV1. As importantly the reported mean values for RAW and SGAW are often inconsistent from one study to another. RAW and SGAW can show significant changes post-bronchodilator or during a methacholine challenge but again these are comparatively much larger than they are for FEV1 and there are no ATS/ERS guidelines for the level of change that should be considered significant.
RAW and SGAW measurements require a body plethysmograph which severely limits which facilities are able to perform these tests, particularly when compared to spirometry. RAW and SGAW measurements are easy to add to the routine measurement of plethysmographic lung volumes but still require careful calibration and attention to detail. Whether or not RAW testing should be performed at all comes down to its perceived clinical utility.
RAW and SGAW may be more sensitive to changes in airway status than FEV1 and at least one study has suggested that airway resistance was abnormal in many patients with asthma who otherwise had a normal FEV1/FVC ratio. But the problem with RAW and SGAW in routine clinical testing is that what’s considered normal, what’s considered abnormal and what’s considered a significant change is still much “fuzzier” than it is for spirometry and this places serious constraints on its clinical relevance.
References:
[A] Briscoe WA, Dubois AB. The relationship between airway resistance, airway conductance and lung volume in subjects of different age and body size. J Clin Invest 1958; 37: 1279-1285
Clausen J. editor. Pulmonary function testing. Guidelines and controversies. Equipment, methods and normal values. Published by Grune & Stratton, 1982.
DuBois AB, Botelho SY, Comroe JH. A new method for measuring airway resistance in man using a body plethysmograph: values with normal subjects and in patients with respiratory disease. J Clin Invest 1956; 35: 327-335.
Greenway SD, Blackwell S, Jhali N, Stenning J, Wilbraham D, Clarke GS. Variability of airway conductance (SGAW) in healthy volunteers. Amer J Respir Crit Care Med 2010; 181: A5003.
[B] Gutierrez C, Ghezzo RH, Abboud RT et al. Reference values of pulmonary function tests for Canadian Caucasians. Can Respir J 2004; 11(6): 414-424.
Krell WS, Agrawal KP, Hyatt RE. Quiet-breathing vs. panting methods for determination of specific airway conductance. J Appl Physiol 1984; 57(6): 1917-1922.
Lord PW, Edwards JM. Variations in airways resistance when defined over different ranges of airflows. Thorax 1978; 33: 401-405.
[C] Marsh S, Aldington S, Williams M et al. Completer reference ranges for pulmonary function test from a single New Zealand population. New Zealand Med J 2006; 119, no. 1244
Miller WF, Scacci R, Gast LR. Laboratory evaluation of pulmonary function. Published by J.B. Lipincott Co., 1987.
Peslin R, Duvivier C, Malvestio P, Benis AR, Polu JM. Frequency dependence of specificic airway resistance in a commercialized plethysmograph. Eur Respir J 1996; 9: 1747-1750.
Ries AL, Clausen J. Chapter: Airway Resistance. Pulmonary function testing indications and interpretation. Wilson AF, editor. Published by Grune & Stratton. 1985.
Topalovic M, Derom E, Osadnik CR, Troosters T, Decramer M, Janssens W. Airways resistance and specific conductance for the diagnosis of obstructive airways diseases. Respir Res 2015; 16: 88.
Topalovic M, Exadaktylos V, Troosters T, Celis G, Aerts J-M, Janssens W. Non-linear parameters of specific resistance loops to characterise obstructive airways disease. Respir Res 2017; 18: 9.