
The single-breath DLCO maneuver can rightly be criticized as being an artificial maneuver that bears little resemblance to normal breathing. It is only by standardizing the maneuver that clinically relevant and reproducible results can be obtained. One important aspect of this standardization is the breath-holding period.
The single-breath DLCO maneuver begins with a subject exhaling to RV, followed by an inhalation of the test gas mixture to TLC and then a 10-second breath-holding period, ending with an exhalation during which a sample of alveolar air is collected. The initial choice of a 10-second breath-hold period was largely arbitrary and was selected in order to strike a balance between being a short enough period that for most patients to hold their breath, long enough to minimize the inspiratory and expiratory phases and long enough to allow for a sufficiently measurable amount of carbon monoxide to be taken up.
During the inspiratory phase of the DLCO maneuver, carbon monoxide uptake does not begin until the inhaled gas has passed both the test system’s and the subject’s anatomic dead space and reached the first functional alveolar-capillary unit. The full rate of carbon monoxide uptake will not occur until the diffusing gas mixture has reached all available alveolar-capillary units and these units have reached their maximum surface area. The rate of carbon monoxide uptake therefore increases throughout inhalation and reaches a maximum near TLC.
During the exhalation phase, carbon monoxide uptake continues even as the alveolar sample is being taken. For this reason the concentration of carbon monoxide at the beginning of the sampling period tends to be higher than at the end of the sampling period. The size of the washout volume and the alveolar sample volume, which to some extent determines how long a patient has to exhale before the acquisition of an alveolar sample is complete, will also have an effect on exhaled gas concentrations.
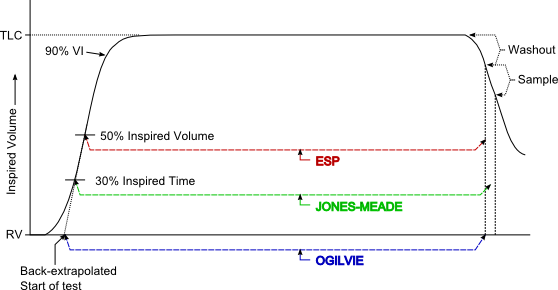
Because the point at which carbon monoxide uptake starts and the point at which it ends are to some degree indeterminate, several methods for standardizing the measurement of the single-breath DLCO breath-hold period have been developed. Of these, the Ogilvie method starts measuring the breath-hold period at the very beginning of inhalation and stops at the beginning of the alveolar sampling period. The Epidemiology Standardization Project (ESP) method, on the other hand, also stops at the beginning of the alveolar sampling period but instead starts measuring at 50 percent of the inhaled volume. Finally, the Jones-Meade method starts measuring at 30 percent of the inspiratory time and stops in the middle of the alveolar sampling period.
As a reminder, single-breath DLCO is calculated by:

A DLCO test measures the rate of CO uptake which is expressed as ml/min/mm Hg. For the same inspired and expired CO concentrations a shorter BHT would mean a quick uptake of CO has occurred and a longer BHT would mean a slow uptake of CO has occurred. When these different breath-hold measurement methods are applied to the same test results, the ESP method, which generates the shortest breath-hold time, has the largest calculated DLCO. The Ogilvie method, which generates the longest breath-hold time, has the smallest calculated DLCO. The Jones-Meade method tends to fall in between the ESP and Ogilvie methods in patients with normal lungs.
Both the Ogilvie and the ESP methods tend to overestimate DLCO when airway obstruction is present. This is because with airway obstruction it takes longer to get an alveolar sample. Both the Ogilvie and ESP methods stop measuring time at the beginning of the alveolar sampling period, even though some CO uptake may still be occurring. For this reason they tend to generate a shorter breath-hold time than may be appropriate. The Jones-Meade method however, includes some of the alveolar sampling time in the measurement of breath-hold time and therefore tends to have the least overestimation of DLCO in the presence of airway obstruction. It is for this reason that the ATS-ERS Statement on DLCO testing recommends the use of the Jones-Meade method.
Both the Ogilvie and Jones-Meade methods for measuring the beginning of the breath-hold period are time based, so it is important to know when inspiration begins and ends. Ideally the onset of inspiration should be rapid and easily recognizable. When it is less easy to determine the beginning of inspiration, the ATS recommends use of the standard back extrapolation technique to determine the onset of inspiration. The end of inspiration should also be clear and easily recognizable. When it is not, the ATS recommends using point at which the inspiratory volume equals 90% of the patient’s vital capacity as the end of inspiration.
Regardless of the method used to measure breath-hold time, the periods of inhalation and exhalation should be kept as short as possible in order to minimize measurement inaccuracies. The formula used to calculate DLCO does not by itself differentiate between the inhalation phase, breath-hold period and the exhalation phase; all are considered to be part of the breath-hold period. Several researchers have devised techniques that calculate and then integrate DLCO for each of these phases. This approach is based on physiological models and is known as the 3-equation method. It is available on some test systems but is not recommended by the ATS or ERS at this time.
As mentioned previously, the choice of a 10-second breath-hold period was somewhat arbitrary. In subjects with normal lungs, DLCO tends to decrease when breath-holding lasts longer than 10 seconds. A variety of potential causes for this have been proposed which include build-up of CO back pressure and changes in circulation but regardless there seems to be little reason to propose a longer breath-holding period. A shorter breath-holding period may be acceptable since at least one study has shown that breath-holding periods of 6 or 8 seconds gives reasonably equivalent results. The problem with shorter breath-holding periods is that inspiration and expiration become a significant part of the overall time period.
These findings apply primarily to subjects with normal lungs however. There is general agreement that patients with COPD show increases in DLCO with longer breath-holding times. For these patients a longer breath-hold time allows more time for axial diffusion and therefore increased ventilation of poorly ventilated lung units as well as a better estimation of VA.
It should also be remembered that the conditions under which the breath-hold period is conducted can also affect the measured DLCO. During the breath-hold period, a Valsalva maneuver (forcible exhalation against a closed airway) acts to raises the intrathoracic pressure thereby decreasing both the pulmonary blood volume and the DLCO. A Muller maneuver (forcible inhalation against a closed airway), on the other hand, decreases intrathoracic pressure, thereby increasing pulmonary blood volume and the DLCO. For these reasons the ATS-ERS Statement on DLCO testing recommends that the patient avoid excessive positive (Valsalva) or negative (Muller) pressure maneuvers during the breath-hold period. Determining whether these have occurred, however, can be difficult. Most DLCO tests system have a valve arrangement that prevents exhalation during the breath-hold period. Some of the test systems my lab uses monitor airway pressure during the breath-hold period but the usefulness of this measurement assumes the patient keeps their airway open during breath-hold and my impression is that most patients close their glottis instead.
There are many approaches towards measuring gas exchange, but the single-breath DLCO has become the primary way of making this measurement. The single-breath DLCO test is an artificial maneuver that nevertheless provides clinically significant information about gas exchange. How the BHT is measured has implications for DLCO calculations and should also be a consideration when choosing DLCO reference equations. Because the BHT includes some or all of the inspiratory and expiratory components of the maneuver it necessarily simplifies a complex situation. The Jones-Meade approach to measuring BHT attempts to minimize these components and is probably a good compromise. Although the choice of a 10 second BHT was fairly arbitrary it also appears to strike a good balance between physiology, patient abilities and test equipment limitations.
REFERENCES:
Beck KC, Offord KP, Scanlon PD. Comparison of Four Methods for Calculating Diffusing Capacity by the Single Breath Method. Chest 1994; 105:594-600
Brusasco V, Crapo R, Viegi G editors. ATS/ERS Task Force: Standardization of Lung Function Testing. Standardization of the single-breath determination of carbon monoxide uptake in the lung. Eur Resp J 2005; 26:720-735
Dressel H, Filser L, Fishcher R, de la Motte D, Steinhaeusser W, Huber RM, Nowak D, Jorres RA. Lung diffusing capacity for nitric oxide and carbon monoxide: Dependence on breath-hold time. Chest 2008; 133:1149-1154
Ferris BG, ed. Epidemiology Standardization Project. Am Rev Resp Dis 1978; 118:6(Part 2;1-120)
Graham BL, Mink JT, Cotton DJ. Overestimation of the Single-Breath Carbon Monoxide Diffusing Capacity in Patients with Air-Flow Obstruction. Am Rev Resp Dis 1984; 129:403-408
Graham BL, Mink JT, Cotton DJ. Effect of breath-hold time on DLCO(SB) in patients with airway obstruction. J Appl Physiol 1985; 58:1319-1325
Jones RS, Meade FA. Pulmonary Diffusing Capacity: an improved single-breath method. Lancet 1:94-95
Lawson WH. Effect of drugs, hypoxia and ventilatory maneuvers on lung diffusion for CO in man. J Appl Physiol 1972; 32:788
Leech JA, Martz L, Liben A, Becklake M. Diffusing Capacity for Carbon Monoxide: The Effects of Different Derivations of Breathold Time and Alveolar Volume and of Carbon Monoxide Back Pressure on Calculated Results. Am Rev Resp Dis 1985; 132:1127-1129
Ogilvie CM, Forster RE, Blakemore WS, Morton JW. A Standardized Breath Holding Technique For The Clinical Measurement Of The Diffusing Capacity Of The Lung For Carbon Monoxide. J Clin Invest 1957; 36:1-17

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.