
When we went through our hardware and software upgrade last August, one of the changes we made was to stop reporting the FEF25%-75% (AKA MMEF, MMFR, MMF). The pulmonary physicians had long since stopped using this value when assessing spirometry results and we had kept it on our reports as long as we did only for inter-laboratory compatibility. Along with other changes we made at that time we decided it was time to drop the FEF25%-75% off our reports.
FEF25%-75% has been used to assess “small airways disease” but more than one of our pulmonary physicians has said that they don’t believe there is such a thing. I’m not a clinician but I’ve always felt that tests and results need to be clinically useful in order to be performed or reported and more than one study has shown little correlation between anatomical findings and FEF25%-75%.
Regardless of whether or not small airways disease is an actual entity my first objection to the FEF25%-75% has to do with the concept that it measures flow in small airways when for most patients it lies within their FEV1. For this reason it has never been clear to me what the FEF25%-75% is measuring that the FEV1 isn’t. More importantly, I have significant concerns about the limitations involved in measuring the FEF25%-75% in the first place.
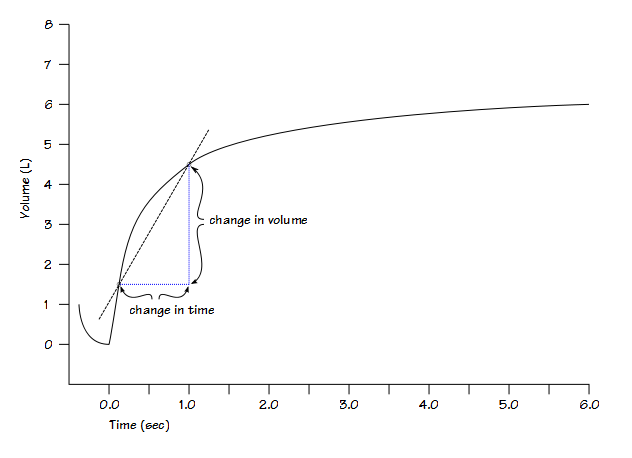
FEF25%-75% is measured by identifying the points at which 25% and 75% of the Forced Vital Capacity has been exhaled and then calculating the change in volume divided by the change in time:
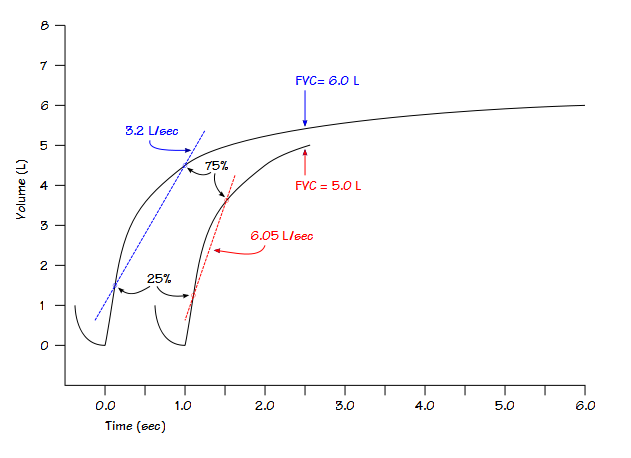
 Using the FVC as the primary reference means that the measured FEF25%-75% is highly dependent on the FVC volume. Getting a truly maximal FVC from patients with lung disease requires a lot of effort and cooperation from the patient. An effort where the FVC is underestimated will cause the FEF25%-75% to be disproportionally overestimated. Small changes in FVC can have large changes in FEF25%-75%.
Using the FVC as the primary reference means that the measured FEF25%-75% is highly dependent on the FVC volume. Getting a truly maximal FVC from patients with lung disease requires a lot of effort and cooperation from the patient. An effort where the FVC is underestimated will cause the FEF25%-75% to be disproportionally overestimated. Small changes in FVC can have large changes in FEF25%-75%.
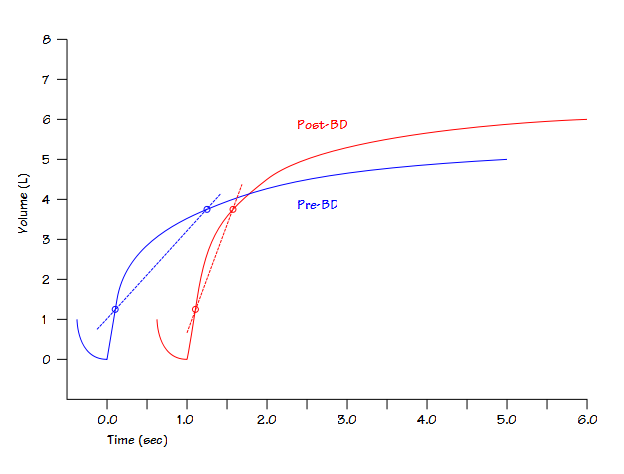
This was also noted when the FEF25%-75% from pre- and post-bronchodilator spirometry efforts were compared. Numerous investigators saw that FVC and FEV1 could increase significantly post -bronchodilator but the FEF25%-75% often did not. The fact is that the FEF25%-75% from the pre- and post-bronchodilator efforts was being measured across a different set of lung volumes whenever the FVC increased post-bronchodilator. The solution has been to measure the post-bronchodilator FEF25%-75% at exactly the same volume points as the pre-bronchodilator effort. This is called volume adjustment and to some extent it makes sense but at the same time it calls into question exactly what the FEF25%-75% is measuring.
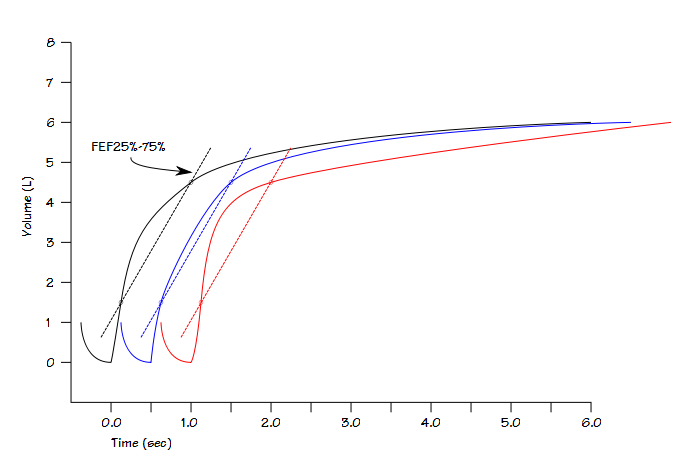
 To be honest, I think that adjusting the FEF25%-75% volume smacks of tweaking the results to meet the expectations. I will agree that there is a general correlation between flow rates and airway size during a forced exhalation but strictly speaking this is what the different flow-volume loop contours are all about. The primary problem with applying this concept to the FEF25%-75% is that the FEF25%-75% is an average flow rate that says nothing about the actual flow rates between the two values used to measure it.
To be honest, I think that adjusting the FEF25%-75% volume smacks of tweaking the results to meet the expectations. I will agree that there is a general correlation between flow rates and airway size during a forced exhalation but strictly speaking this is what the different flow-volume loop contours are all about. The primary problem with applying this concept to the FEF25%-75% is that the FEF25%-75% is an average flow rate that says nothing about the actual flow rates between the two values used to measure it.
Since the FEF25%-75% lies within the FEV1 it is not surprising that it correlates well with airway obstruction. The correlation between FEV1/FVC ratio and FEF25%-75% is actually too good because at least one study showed that FEF25%-75% is always normal when the FEV1/FVC ratio is normal. This brings into question what additional information the FEF25%-75% adds, if any, towards assessing spirometry results.
As an alternate to FEF25%-75% some investigators have suggested that FEV3 and the FEV3/FVC ratio provides a much better window onto small airways. I did a pilot study on a few hundred patients using the FEV3/FVC ratio with ambiguous results. I found that like the FEF25%-75% the FEV3/FVC ratio was abnormal when the FEV1/FVC ratio was normal only rarely. It may be possible that with a larger sample of patients the FEV3/FVC can serve a purpose but so far none of our pulmonary physicians have shown an interest in it so its value remains speculative to me.
Our lab software is able to report over two dozen different values from a single forced vital capacity. Most of these values are not clinically useful. The FEF25%-75% has high inter-test and intra-test variability and is unduly affected by FVC. Given the limitations in how and what it measures it is not clear to me that the FEF25%-75% has much to do with identifying the site of airway obstruction. It is also unlikely that it provides any information not already provided by the FEV1 and FEV1/FVC ratio. I think it is time that everyone should think about dropping the FEF25%-75% from their reports too.
References:
Berend N, Wright JL, Thurlbeck WM, Marlin GE, Woolcock AJ. Small airways disease: Reproducibility of measurements and correlation with lung function. Chest 1981; 79: 263-268
Cockcroft DW, Berscheid BA. Volume adjustment of maximal midexpiratory flow. Importance of changes in Total Lung Capacity. Chest 1980; 78: 595-600
Gelb AF, Williams AJ, Zamel N. Spirometry. FEV1 vs FEF25-75 percent. Chest 1983; 84: 473-474
Hansen JE, Sun XG, Wasserman K. Discriminating values and normal values for expiratory obstruction. Chest 2009; 136: 369-377
Sherter CB, Connolly JJ, Schilder DP. The significance of volume-adjusting the maximal midexpiratory flow in assessing the response to a bronchodilator drug. Chest 1978; 73: 568-571

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.