
While reviewing reports today I ran across a couple of lung volume tests from different patients where the SVC was over a liter less than the FVC. Suboptimal SVC measurement can affect both the TLC and the RV and in one case the TLC was slightly below normal (78% of predicted) and in the other the TLC was within normal limits but the RV was over 150% of predicted. Both patients had had lung volume measurements previously and the current TLC was significantly different than it had been before.
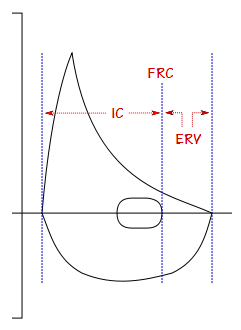
I seem to run across this problem at least once a week so I am reasonably used to making manual corrections. I’ve discussed this previously but basically I use the position of the tidal loop within the maximal flow-volume loop obtained during spirometry to determine IC and ERV and then re-calculate TLC and RV accordingly.
Anyway, for this reason I had tidal loops, and IC and ERV on my mind while I was reviewing other reports. Shortly after this I came across a report that had “fair FVC test quality and reproducibility” in the tech notes so I pulled up the raw spirometry test data and took a closer look.
What I found was that the patient had performed five spirometry efforts and that the FVC and FEV1 was different on each test. All five spirometry efforts met the ATS/ERS criteria for back-extrapolation, expiratory time and end-of-test flow rates. I clicked back and forth between the different spirometry efforts to make sure the right FVC and FEV1 had been selected and when I did I noticed that the position of the tidal loop was shifting left and right and that the closer it was to TLC, the lower the FVC and FEV1 were and vice versa.
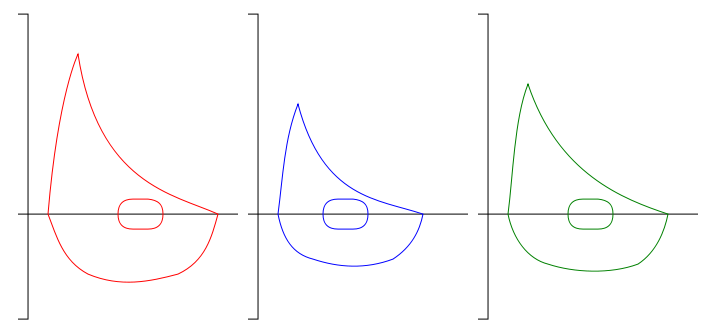
We almost never use IC and ERV when talking about spirometry, but using the end-exhalation of the tidal loop as a marker for FRC I noticed that the ERV was pretty much the same for all efforts and that it was the IC that was changing the most. This told me that although the patient was likely exhaling completely with each effort, their inspiration wasn’t as maximal as it should have been every time.
Almost all of the ATS/ERS criteria for assessing the quality of a spirometry effort (i.e. back extrapolation, expiratory time, end of test flow rates) are oriented towards a maximal exhalation. But other than stressing that the FVC maneuver should start from TLC (i.e. a maximal inspiration) there are no criteria whatsoever for assessing the quality of an inspiratory effort. In a sense this is not surprising since there is nothing in particular in a flow-volume loop or volume-time curve that can indicate that an inspiration has truly been maximal.
In this instance however, when the spirometry efforts were compared with each other the change in IC was a strong indicator for the quality of each effort’s inspiration. By itself IC can’t be the sole indication of a maximal inspiration, but I can’t help but think that if the technician performing the test was aware that IC was changing while ERV was remaining fairly constant that they would have spent more time coaching the patient on the inspiratory part of the maneuver. But IC and ERV aren’t measured from an FVC maneuver and as importantly, the conventions that are used when displaying flow-volume loops makes it difficult to see changes in these values.
Specifically, although our lab software (and probably the software from most of the other manufacturers of spirometers and lab systems) can overlay the flow-volume loops from different spirometry efforts the standard convention is to position the flow-volume loops using the maximum inspiration of each effort.
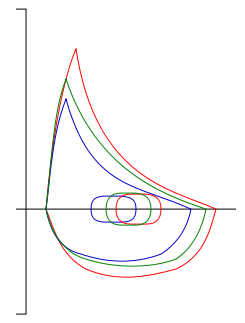
When flow-volume loops are displayed this way it’s hard to compare the IC and ERV from each effort even if you have a really good eye. But if flow-volume loops were positioned according to the end-exhalation of the tidal loops, IC and ERV would become much more apparent.
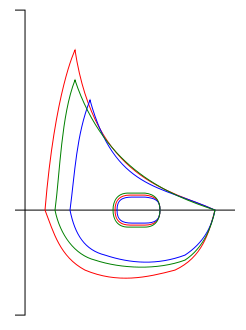
Using IC and ERV to help assess the quality of spirometry maneuvers would require some changes in the way that we think about the test. Strictly speaking however, even though measuring the numerical values for IC and ERV would be useful, all that’s really necessary is to change the way flow-volume loops are displayed (or at least have the option) since that alone would make the differences more evident.
I fully understand why IC and ERV should be measured from a slow VC when lung volumes are being calculated. Relaxed and stable tidal breathing is needed for a repeatable FRC and the steady effort of an SVC maneuver is needed to obtain accurate and repeatable IC and ERV measurements. Tidal breathing is not included in the ATS/ERS spirometry standards and strictly speaking the quality of any pre-maneuver tidal breathing is not a necessary component towards obtaining a quality FVC.
Having said that, I’ve always felt that starting an FVC maneuver with a couple tidal breaths was one way to to make sure the patient wasn’t leaking around the mouthpiece and it also lets me cue them better for the FVC maneuver. I have almost always started the FVC with at least a couple tidal breaths and this is the approach I have always taught to others. So for me at least, as well as most of the spirometry performed in my lab (and I suspect many other labs as well), tidal loops are usually included with each FVC effort.
Given the circumstances surrounding the FVC maneuver I suspect that the IC’s and ERV’s obtained from an FVC are likely less repeatable and more variable than those obtained from an SVC but interestingly enough however, I’ve never seen any study that looked at this or at the repeatability of the IC and ERV from SVC maneuvers, so this will have to remain speculation on my part.
Looking back at my original problem (the one that got me thinking about tidal loops, IC and ERV in the first place) having a numerical value for IC and ERV from the FVC would make it easier to re-calculate lung volumes. As importantly I’ve seen lab software where the FVC was automatically substituted for the SVC when it was larger, but a distinct problem with this approach is how the FVC is inserted into the lung volume calculations. Since IC and ERV aren’t measured from the FVC maneuver what usually happens is that the RV calculated using the ERV from the original SVC is retained (no matter how bad the SVC was) and a new TLC is calculated from the FVC and RV. Since the SVC is being replaced in these circumstances because it is underestimated to begin with (and at a guess the ERV is more likely to have been underestimated and RV overestimated) then calculating a TLC using a questionable RV means the TLC will also be questionable. This is where having an IC and ERV from the FVC maneuver are more likely to lead to a more accurate RV and TLC than using the IC or ERV from the SVC it’s replacing.
We’re not used to thinking about IC and ERV in conjunction with spirometry but whenever an FVC maneuver is preceded by tidal breathing it’s possible to measure IC and ERV. Making the IC and ERV more visually apparent by positioning flow-volume loops based on the end-exhalation of the tidal loop and not the maximal inspiration gives additional information about the quality of a patient’s inspiratory and expiratory efforts that is not presently available. For this reason I’d like to see this as an option when overlaying spirometry efforts during testing. I’d also suggest that the next time the ATS/ERS revises the standards for spirometry that tidal breathing, at least an option, should be included as part of the FVC maneuver.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License